By any measure, some minimal level of healthcare is important for sustainable economic development. About 50 million Indians live every year at risk of being pushed into poverty by healthcare expenses. We know a lot about the Indian healthcare system in a top-down sense and we have some vignettes of what it's like at the bottom. Most experts suggest that many of its problems are because of low government spending.
But if everyone agrees that higher government spending in health and education is the answer, why hasn't the government done it? The NDA government seems very committed - at least rhetorically - to high economic growth, and a broader middle class with more education and less mortality seems to be generally a good step in that direction. What's the disconnect here, and why hasn't policy shifted? Too much research talks about the fact that government spending is low and fails to ask why this is the case. More generally, the incentives within the institutional structures of government are undertheorized. This seems like an appropriate case for Progress Studies!
I wrote up a blog post on some challenges to this. It's available here on my Substack and is cross-posted below:
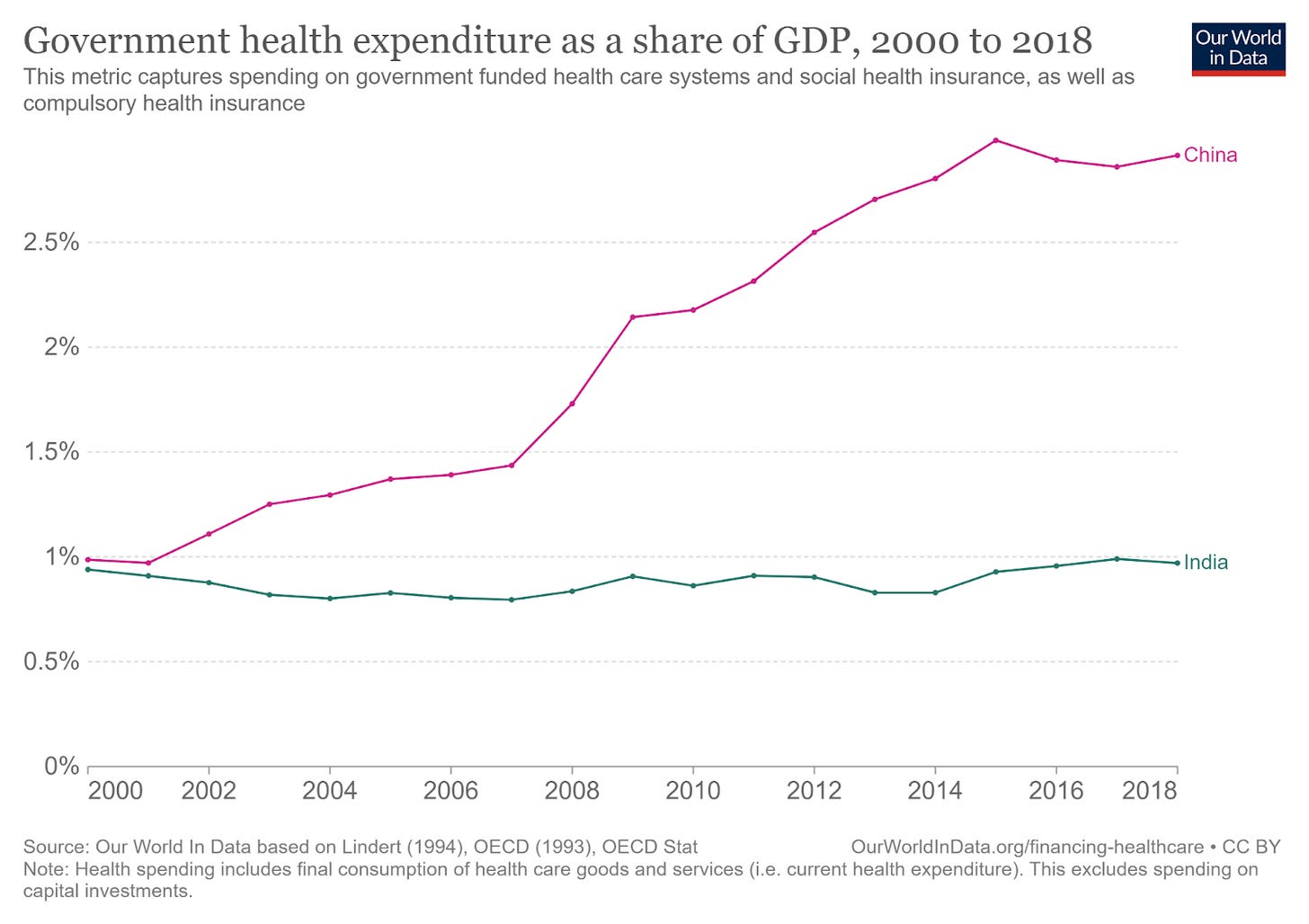
Source: Our World in Data (link)
I.
Governments usually spend more on healthcare as they become richer. Between 2000-2018, India’s GDP grew from $468 billion to $2.7 trillion. In the same period, Chinese Government Health Spending (GHS) grew from one percent to nearly three percent of GDP. In India, however, GHS stagnated at around one percent.
As a result, India has one of the lowest public health budgets in the world relative to the size of its economy. But why? Health and education, Amartya Sen keeps telling us, are central to sustained economic growth. This is, of course, a product of the slightly important fact that people end up living longer, healthier lives. Why wouldn’t India want a thriving, healthy middle class and profit from that demographic dividend everyone keeps talking about?
Let’s start by breaking down health spending.

Source: National Health Accounts Estimates for India, Published November 2018 (link)
Most healthcare costs are paid by patients out of pocket, and most of that goes to medicines, diagnostics, and ambulatory care (which is the healthcare you get without being admitted to a hospital). Formal insurance schemes make up less than a tenth. Public health spending (the states and the central government combined) makes up less than a third of the total health expenditure in India.
II.
Why is public health spending so low, despite the burden that healthcare costs put on households? One idea is that the Indian state simply does not care. Inspired by Boris Johnson, we will call this the Let The Bodies Pile High view – in which the Indian government does not particularly care about the destitute masses. It goes like this: the Indian government has neoliberal economic views, has only apathy for the poor, or simply does not believe it is the role of government to enact social good. I am ambivalent about these arguments. I am going to try to see if there is an answer besides apathy.
While India is not particularly spendthrift – government spending was only about 18% of GDP in 2021 – we do have massive food and fertiliser subsidies. Health just doesn’t seem to be a big priority. Sujatha Rao (Do We Care?, 2016), who we will rely on extensively, blames economists for this. The post-independence Nehruvian Model emphasised economic planning and development, and particularly focused on self-sufficiency and reducing imports. The government focused aggressively on irrigation, agriculture, and power plants and neglected education and health in the process. While China was launching massive campaigns for behaviour change, hygiene, and sanitation, India stuck to a narrow public health agenda limited to family planning and malaria prevention.
Maybe the government is simply leaving the market to its devices. Did private providers expand to fill the gap created by the absence of the state? Contrary to popular perception, private healthcare is not merely available to the wealthy. In rural India, “most providers are in the private sector (86 per cent).” These private providers are usually unqualified – with no formal training. However, it turns out (from a 2010-11 study in rural Madhya Pradesh and urban Delhi) that “private practitioners with no formal training were as likely to diagnose correctly as qualified doctors in government hospitals.” But If government doctors are as bad as unqualified providers, that is a failure of medical education, not the success of the market. The private sector can provide healthcare, and they fill a massive gap, but not at a low enough cost to meet the needs of India’s poorest. And the private sector can’t do massive public health programmes or invest in preventive care.
III.
Why haven’t the States invested heavily in healthcare? Some have, and they’re mostly southern states like Kerala and Tamil Nadu. You can’t give social democracy all the credit - these states had serious advantages and still incurred serious costs. People in Kerala largely settle in small towns which are somewhat proximate to each other, making it much easier to get over physical distance and reducing inequalities between urban and rural areas, one of the biggest barriers to healthcare access. Kerala’s government was very willing to throw out fiscal discipline, take on debt, and aggressively invest in people’s well-being all the way until they ended up in a multi-decade fiscal crisis. By that point, however, infrastructure had developed sufficiently, an epidemiological transition had taken place, and the private sector could take it from there.
In some states, like Bihar or Uttar Pradesh, the answer is just poverty. On average, according to Rao, states need to “almost treble their spending from the current level of 2.4% to 8%.” This is very difficult, because the states that are bad at public health also don’t have enough money. Rao writes: “Three-quarters of disease burden is concentrated in about nine states that also account for an equal number of the poor.” Additionally, the “per capita income ratio between them and the better-off states is 1:5, making it impossible for any central government to bridge the divide.” Those who most need to spend cannot and those who can really don’t need to.
You simply cannot get around poverty. You cannot redistribute your way out of your problems unless you get to a minimum level of GDP-per-capita. Whatever that minimum is, it‘s higher than Uttar Pradesh’s measly $860. For reference, the Indian average in 2019 was $2100 and Kerala’s in 2021 was $3100. Rao says that the capital investment necessary to bridge this gap would require a hike in the tax-to-GDP ratio by at least 20 percent. And the government can’t raise taxes or introduce copayments or fees because almost everyone (93%) works in the informal sector and about 40% of them have “no assets or steady incomes.” There’s also an enormous failure of medical education. Credentials are not predictors of quality in poorer states: qualified doctors in Bihar scored lower than unqualified providers in Kerala.
IV.
Why are some states so much better off than others? Rao blames the federal division of powers for this. While the States and the Union can both legislate on relatively inexpensive areas like drug regulation or statistical collection, only the States are empowered to deal with public health, sanitation, hospitals, and dispensaries. This division of powers condemns the States to perpetual fiscal insecurity and makes them dependent on the Union for grants. Some revenues are collected by the Union and shared with the States, and the precise split is managed by the Finance Commission, which has almost never made health a priority. If the Union doesn’t make health a priority, the States will have to do so. And as we have seen, there are various reasons why the States can’t, or at least find it very difficult.
Let’s assume the availability of funds wasn’t an issue and skip ahead to the final boss: the Indian government’s hard-won reputation for centralised slowness and elephantine bureaucracy, which delays the release of funds and withholds approved budgets. Rao describes, with evident frustration, how short-termism is baked into the operating protocols of the Indian state. Quarterly accounting has been elevated to a priesthood that takes precedence over actual health outcomes. In some instances, approval would be granted by a bureaucrat who would, minutes later, call up the finance department and tell them not to sanction the necessary funds.
V.
To sum up, It’s not just expensive, but also incredibly hard to spend on health in a way that moves the needle. Policymakers and administrators face a complex, labyrinthine bureaucracy, as well as an inflexible constitutional structure that is allergic to long-term thinking. These factors condemn parts of India to generational poverty, illiteracy, and ill health.
I leave you with this: if a democratic state doesn’t actively try to prevent about fifty million of its people from having to choose, every year, between poverty and death - what are we to call such a state? I’m not sure I have a better answer than “apathetic.” Nevertheless, I have delivered on my reductionist premise that these things are not as simple as apathy. But, my dear reader, what on earth gave you the idea that apathy was simple?
In the next post, we will look at Centre and State expenditures and find out where the money is going instead. We will also spend a lot of time on states like Bihar, Uttar Pradesh, and Madhya Pradesh which have poor healthcare and compare them with the health budgets of states like Kerala.
Pradyumna Prasad, Akshay, Nithya, Akshay Dinesh, and Sanjana reviewed early drafts and improved this post substantially with their helpful comments.
If I haven’t linked to a fact or statistic in the body text, it’s from one of the following books:1